My Heart Beats Then There Is a Large Pause Then It Goes Back to Beating Normally Again
Overview
The Normal Heart Charge per unit
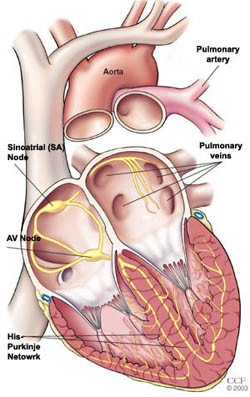
The heart's rhythm is coordinated by its own electrical arrangement. With each heartbeat, the electrical impulse begins at the sinus (or sinoatrial, SA) node, too called the heart'south natural pacemaker. The SA node is a cluster of specialized cells, located in the right atrium. The SA node produces the electrical impulses that set the charge per unit and rhythm of your heartbeat. The impulse spreads through the walls of the right and left atria, causing them to contract, forcing blood into the ventricles.
The Heart'south Electrical Organisation
The impulse then reaches the atrioventricular (AV) node, which acts every bit an electrical bridge allowing impulses to travel from the atria to the ventricles. In that location is a short filibuster before the impulse travels on to the ventricles. From the AV node, the impulse travels through a pathway of fibers called the HIS-Purkinje network. This network sends the impulse into the ventricles and causes them to contract. The contraction forces blood out of the centre to the lungs and body.
The SA node fires another impulse and the cycle begins once more.
The heartbeat is triggered past electrical impulses that travel downwardly a special pathway through your heart muscle.
Heart Charge per unit and Rhythm Differences Between Men and Women
Women and men are similar when it comes to the basic centre charge per unit and rhythm. However, while the basic electrical arrangement is the same (impulses originating in the SA node, traveling to the AV node, through the HIS-Purkinje, and then starting over), in that location are differences:
- Women tend to have a faster baseline center rate
- Women'southward ECG readings may be different
Women Have a Faster Baseline Heart Rate Than Men
Showtime of all, on average, women tend to accept a faster baseline heart rate than men. This difference is seen in girls, on an average, as young as five years old. At that place is besides a shorter sinus node refractory time – this means that it takes a shorter time for the SA node to recover and become fix to fire an impulse again ¹
Women's ECG Readings may be Unlike
The ECG (also called EKG or electrocardiogram) is a exam used to record on graph paper the electrical activeness of the heart. The motion picture, drawn by a computer from information supplied by electrodes placed on the skin of the breast, arms and legs, shows the timing of the different phases of the heart rhythm.
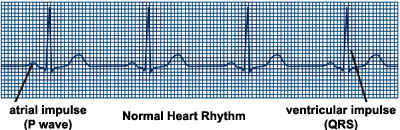
The p wave represents the electric activity of the upper chambers of the heart (atria). There is a short pause followed by the QRS complex - the electrical activity of the lower chambers (ventricles) - and ends with a small T wave, the recovery phase of the ventricles. The QT interval is the distance from the beginning of the QRS to the end of the T wave and represents the time information technology takes for the center muscle to contract and then recover, or for the electrical impulse to burn and then recharge.
On average, the QT interval is shorter in men than in women, beginning after puberty with a linear increment through the major part of adulthood to at to the lowest degree age 55. This period corresponds to the time menstruum when androgen levels are highest in men. Therefore, androgen and estrogen levels may explain the gender differences in QT interval².
- Taneja T, Mahnert BW, Passman R, Goldberger J, Kadish A. Effects of sex and historic period on electrocardiographic and cardiac electrophysiological properties in adults. Pacing Clin Electrophysiol. 2001 January;24(1):16-21.
- Rautaharju PM, Zhou SH, Wong S, Calhoun HP, Berenson GS, Prineas R, Davignon A. Sex activity differences in the evolution of the electrocardiographic QT interval with age. Can J Cardiol. 1992 Sep;8(7):690-v.
Certain types of arrhythmias are more than prevalent in women than in men.
These include:
- Supraventricular Tachycardia (SVT) or Paroxysmal SVT (PSVT) – a rapid heart charge per unit that originates above the AV node, in the atria. SVT is mutual in both men and women, but more women accept AV node reentrant tachycardia and atrial tachycardia¹.
- Sinus Node Dysfunction (also chosen sick sinus syndrome) – a slow or irregular centre rhythm that originates in the SA node. The betoken starts in the SA node simply may be slow or delayed in progressing to the atria, causing a very deadening or irregular heart beat.
- AV Nodal Re-entry Tachycardia (AVNRT) - a type of SVT with a fast heart rate that originates in the AV node. Instead of the AV node sending the impulse downward 1 pathway, there are two pathways through the AV node. The impulses travel through one pathway as well as back upward through the second pathway. This allows the impulses to travel around the AV node very quickly in a circular style, causing the heart to trounce unusually fast.
- Long QT Syndrome - a QT interval longer than normal. This increases the adventure for life-threatening forms of ventricular tachycardia.
- Postural Orthostatic Tachycardia Syndrome (POTS) - a condition that affects 500,000 Americans, primarily women. Those with POTS have an abnormal response to alter in position, related to the autonomic nervous arrangement, causing drop in blood pressure, raise in heart rate and sometimes syncope (passing out), dizziness or lightheadedness².
These arrhythmias occur more frequently in men, just may present differently in women:
- Atrial Fibrillation - one of the most common irregular center rhythms. It is a rapid irregular heart rhythm originating in the atria. Men have atrial fibrillation more oft than women. Atrial fibrillation can be associated with other types of heart disease. Women are more likely to have atrial fibrillation associated with valve disease, while men more than often have atrial fibrillation associated with coronary avenue disease. The incidence of atrial fibrillation increases in both men and women with age, and when they besides have hypertension and diabetes. The Copenhagen Eye Report showed that women with atrial fibrillation had an increased risk for stroke and cardiovascular expiry as compared to men. This is specially true in women who have atrial fibrillation and are older than age 75 ³ ⁴. Women who have paroxysmal atrial fibrillation, a type of atrial fibrillation that is intermittent (or comes and goes), may have a faster heart rate response than men, and tend to have longer episodes ⁵.
- Sudden Cardiac Death is a sudden, unexpected death caused past loss of eye function (sudden cardiac arrest). Sudden cardiac death (SCD) occurs less oftentimes in women, but is still related to most 400,000 deaths per yr in women. The Nurses' Health Study showed that while the majority of women who had SCD had no prior history of cardiovascular disease before decease, they had at least i cardiac risk factor (smoking, hypertension and diabetes had the greatest bear on). Family history likewise played a function in increased risk if i parent died of middle disease before age lx. The study likewise showed that as with men, the majority of SCD in women was related to an abnormality of the heart rhythm (88%) 5-seven. This reinforces the need for careful screening of heart disease risk factors in women and managing these concerns even without symptoms present.
- Michael J. Porter, Physician, Joseph B. Morton, MBBS, Russell Denman, MBBS, Albert C. Lin, Dr., Sean Tierney, Medico, Peter A. Santucci, Doc, John J. Cai, MD, Nathaniel Madsen, MD, David J. Wilber, Medico. Influence of historic period and gender on the mechanism of supraventricular tachycardia. Eye Rhythm one:four. Oct, 2004, pp: 393-396.
- National Dysautonomia Research Foundation, world wide web.ndrf.org/orthostat.htm .
- Kael WB, Wolf PA, Benjamin EJ, Levy D Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998 Oct xvi;82(8A):2N-9N.
- Friberg J. Comparison of the impact of atrial fibrillation on the risk of stroke and cardiovascular death in women versus men (The Copenhagen Urban center
- Hnatkova Thousand, Waktare JE, Murgatroyd FD, Guo X, Camm AJ, Malik M. Age and gender influences on rate and duration of paroxysmal atrial fibrillation. Pacing Clin Electrophysiol. 1998 Nov;21(11 Pt 2):2455-eight.
- American Heart Clan Center Disease and Stroke Statistics 2012 Update.
- Christine M. Albert, Claudia U. Chae, Francine Grodstein, Lynda K. Rose, Kathryn M. Rexrode, Jeremy N. Ruskin, Meir J. Stampfer, and JoAnn East. Manson. Prospective Report of Sudden Cardiac Death Among Women in the United States. Apportionment, Apr 2003; 107: 2096 – 2101.
Symptoms and Causes
Symptoms of Irregular Centre Rhythms
An arrhythmia may be "silent" and non cause whatever symptoms. A dr. tin detect an irregular heartbeat during an examination by taking your pulse, listening to your heart or performing diagnostic tests.
If symptoms occur, they may include:
- Palpitations – a feeling of skipped heart beats, fluttering, "flip-flops" or feeling that the heart is "running away"
- Pounding in the chest
- Dizziness or feeling light-headed
- Shortness of breath
- Breast discomfort
- Weakness or fatigue (feeling very tired)
Symptoms of palpitations represent 15-25 percent of all the symptoms reported by female person heart patients. They are associated with:
- Premenstrual syndrome
- Pregnancy
- Perimenopausal period
When palpitations are nowadays, the doctor begins his or her evaluation by looking for underlying middle disease. The importance of palpitations and the need for treatment is determined past the presence of underlying heart affliction, the type of irregular eye beats that are occurring and other symptoms that are nowadays.
Hormones and Irregular Centre Beats
Estrogen and progesterone levels rise and fall in women with a normal menstrual cycle during the days of the month. The rising of progesterone and the fall of estrogen correspond with:
- More than frequent episodes of supraventricular tachycardia (SVT)
- More than symptoms associated with SVT
- SVT of longer elapsing¹
During perimenopause (the time menses before menopause), in that location is a marked decrease in ovarian estrogen production. This is associated with an increase in centre charge per unit (sinus tachycardia) and an increased frequency in palpitations and not-threatening arrhythmias, such as premature ventricular contractions or PVCs.
Menopause causes a farther pass up in estrogen as the menstrual cycle stops. This time menstruation is associated with irregular eye beats, palpitations, spasmodic breast pain and nightmares in women 40 -64 years old².
The Heart and Estrogen/Progestin Replacement Study (HERS) institute no do good in the use of hormone replacement therapy to reduce cardiovascular events, and hormone replacement therapy may even increase the gamble of thromboembolism (blood clot) during the first year³. HRT is also associated with lengthening the QT interval [link to the explanation higher up], although the relevance of this finding is not known⁴. On the other manus, HRT may decrease palpitations and other symptoms such as hot flashes, insomnia, and sweating. Therefore, it may be considered a treatment choice in low take chances female patients to relieve symptoms of palpitations.
- Rosano GM, Leonardo F, Sarrel PM, Beale CM, De Luca F, Collins P. Cyclical variation in paroxysmal supraventricular tachycardia in women. Lancet. 1996 Mar 23;347(9004):786-viii.
- Asplund R, Aberg HE Nightmares, cardiac symptoms and the menopause. *Climacteric*. 2003 Dec;6(4):314-20.
- Grady D, Herrington D, Bittner V, Blumenthal R, Davidson M, Hlatky Thou, Hsia J, Hulley S, Herd A, Khan S, Newby LK, Waters D, Vittinghoff E, Wenger Due north; HERS Enquiry Group. Cardiovascular disease outcomes during 6.viii years of hormone therapy: Heart and Estrogen/progestin Replacement Study follow-upward (HERS II). *JAMA*. 2002;288:49-57.
- Gokce K, Karahan B, Yilmaz R, Orem C, Erdol C, Ozdemir S. Long term effects of hormone replacement therapy on center rate variability, QT interval, QT dispersion and frequencies of arrhythmia. *Int J Cardiol*. 2005 Mar thirty;99(3):373-ix.
Arrhythmias & Pregnancy
Premature atrial beats occur in about fifty per centum of women during pregnancy, although most are harmless and exercise not last¹. While sustained arrhythmia is somewhat rare, for those who have supraventricular tachycardia or paroxysmal SVT, the symptoms are worsened in 20 percent of cases¹. Symptoms of SVT may include shortness of jiff, palpitations, and dizziness². Arrhythmias may occur more frequently during pregnancy due to changes in hormones, changes in associated hemodynamic, hormonal and autonomic changes and changes in circulating blood volume, sleep, and emotion during pregnancy.
Women who have had built eye defects repaired accept an increased take chances of arrhythmias during pregnancy. In 27 women who had repaired built heart defects and 29 pregnancies, SVT occurred in xv, ventricular tachycardia in nine, high </ course center block in four and sick sinus syndrome in three women³.
Arrhythmias in pregnancy are treated conservatively. Afterward determining the type of arrhythmia, the physician volition evaluate for underlying causes. If symptoms are minimal, rest and vagal maneuvers may be used to help slow the heart rate. Vagal maneuvers include carotid massage applying ice to the face up, and the Valsalva maneuver, which is the near successful in stopping tachycardias⁴. The Valsalva maneuver involves a person exhaling forcibly with a closed glottis (the windpipe) then that no air exits through the mouth or nose as, for example, in strenuous coughing, straining during a bowel movement or lifting a heavy weight.
When the arrhythmia causes symptoms or a drop in blood pressure, antiarrhythmic medications may be used. No anti-arrhythmic medication is completely safe during pregnancy; therefore medications are avoided during the get-go trimester if possible to limit risk to the fetus. Drugs with the longest safety tape should exist tried get-go. Propranolol, metoprolol, digoxin, and adenosine have been tested and shown to exist well tolerated and safe during the 2d and 3rd trimester⁵.
Cardioversion is safe during all trimesters of pregnancy and tin can be used if necessary¹. In addition, women who take an ICD who go pregnant practice not take an increased gamble for ICD discharges or ICD complications. A woman who has an ICD can safely become pregnant unless she has an underlying heart condition that would increase wellness risks during pregnancy⁶.
- Blomstrom-Lundqvist C, Scheinman MM, et. al. ACC/AHA/ESC guidelines for the direction of patients with supraventricular arrhythmias – executive summary: a report of the American College of Cardiology/American Heart Association Task Strength on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for the Direction of Patients With Supraventricular Arrhythmias). Circulation. 2003 October 14;108(15):1871-909.
- K. Robins\ and K. Lyons. Supraventricular tachycardia in pregnancy. _British Journal of Anaesthesia*, 2004, Vol. 92, No. 1 140-143._
- Tateno Southward, Niwa K, Nakazawa M, Akagi T, Shinohara T, Usda T; A Study Group for Arrhythmia Late after Surgery for Built Heart Disease (ALTAS-CHD). Circ J. 2003 Dec;67(12):992-7.
- Zu-Chi Wen, MD; Shih-Ann Chen, Md; Ching-Tai Tai, MD; Chern-En Chiang, Dr.; Chuen-Wang Chiou, Physician; Mau-Song Chang, MD. Electrophysiological Mechanisms and Determinants of Vagal Maneuvers for Termination of Paroxysmal Supraventricular Tachycardia Circulation. 1998;98:2716-2723.
- Ferrero S, Colombo BM, Ragni Northward Maternal arrhythmias during pregnancy. Arch Gynecol Obstet. 2004 May;269(4):244-53.
- Natale A, Davidson T, Geiger MJ, Newby M. Implantable cardioverter-defibrillators and pregnancy: a condom combination? Circulation. 1997 Nov four;96(9):2808-12.
Diagnosis and Tests
How are arrhythmias diagnosed?
If y'all have symptoms of an arrhythmia, you should make an appointment with a cardiologist. You may want to choose an electrophysiologist, a cardiologist who has received additional specialized grooming in the diagnosis and treatment of heart rhythm disorders.
After evaluating your medical history and discussing your symptoms, a physical test will be performed. The cardiologist also may perform a variety of diagnostic tests to help ostend the presence of an arrhythmia and make up one's mind its causes.
Some tests that may be done to confirm the presence of an irregular heart rhythm include:
- ECG
- Ambulatory Monitor
- Stress Exam
- Echocardiogram
- Electrophysiology Test
- Head Upright Tilt Test
Direction and Treatment
Management of Irregular Eye Rhythms in Women
Treatment options include:
Medications – antiarrhythmic drugs are medications used to convert the arrhythmia to normal sinus rhythm or to prevent arrhythmia. Other medications may include eye-rate control drugs; anticoagulant or antiplatelet drugs such as warfarin (a "blood thinner") or aspirin, which reduce the gamble of blood clots or stroke.
Concerns for women: Because women have a longer QT interval than men. some medications that are used in men to treat irregular heart rhythms prolong the QT interval even more than. These medications include Quinidine, Sotalol, Dofetilide, and Amiodarone. These medications may increase a woman's risk of developing a life-threatening arrhythmia (torsades de pointes) more than in men who take these medications. Women who take these medications should follow their' doctor's and dietitian's dietary guidelines for potassium and avert becoming depression in potassium, which enhances the arrhythmia touch¹.
The biggest concern for all patients with atrial fibrillation is preventing blood clots or stroke. Warfarin (besides called Coumadin) is most often used to prevent strokes in patients. Co-ordinate to The Canadian Registry of Atrial Fibrillation (CARAF), women were half as likely to exist prescribed warfarin as compared to men, although they would benefit from information technology equally much².
Lifestyle changes– arrhythmias may be related to certain lifestyle factors. Here are some ways to change these factors:
- If yous smoke, finish. Acquire More than
- Limit your intake of alcohol. Larn More
- Limit or stop using caffeine. Some people are sensitive to caffeine and may notice more symptoms when using caffeinated products (such every bit tea, coffee, colas, chocolate and some over-the-counter medications).
- Avert certain stimulants. Beware of stimulants used in cough and cold medications and herbal or nutritional supplements. Some of these substances comprise ingredients that cause irregular eye rhythms. Read the label and ask your physician or pharmacist what medication would be all-time for you.
Invasive Therapies – the following invasive therapies may be used to treat or eliminate irregular centre rhythms. Your doctor will discuss the benefits and risks of these therapies and whether they are appropriate treatments for your status.
- Electrical cardioversion – in patients with persistent arrhythmias (such as atrial fibrillation), a normal rhythm may non be achieved with drug therapy alone. After administering a short-acting anesthesia, an electrical shock is delivered to your chest wall that synchronizes the heart and allows the normal rhythm to restart.
- Catheter ablation – during ablation, energy is delivered through a catheter to tiny areas of the heart muscle. This free energy tin either "disconnect" the pathway of the aberrant rhythm; block the abnormal pulses and promote normal conduction of impulses; or disconnect the electric pathway between the atria and the ventricles.
- Pulmonary vein antrum isolation (PVI) – This process is used to treat atrial fibrillation. During PVI, special catheters are inserted into the heart (catheters are inserted into the correct atrium and into the left atrium). Intracardiac echocardiography is used to visualize the left atrium during the procedure. I catheter in the left atrium is used to map or locate the abnormal impulses coming from the pulmonary veins. The other catheter is used to deliver the radiofrequency energy to ablate or create lesions exterior the pulmonary veins. The procedure is repeated for all four pulmonary veins. The lesions form a circumferential scar around the pulmonary veins. The scar blocks any impulses firing from within the pulmonary veins, thereby "disconnecting" the pathway of the abnormal rhythm and potentially curing atrial fibrillation.
Electrical devices – a small device may exist implanted under the skin that can detect an irregular heart rhythm and/or care for it. Your doc will talk over the benefits and risks of implantable devices and whether they are an appropriate treatment for your status.
- Permanent pacemaker – a device that sends small electrical impulses to the center muscle to maintain a normal heart rate. The pacemaker has a pulse generator (which houses a battery and a tiny computer) and leads (wires) that send impulses from the pulse generator to the heart muscle, as well every bit sense the center'south electrical activity. Pacemakers are mostly used to prevent the heart from beating likewise slowly. Newer pacemakers have many sophisticated features that are designed to help with the management of arrhythmias, optimize heart-rate-related functions and better synchronization.
- Implantable cardioverter-defibrillator (ICD) – a sophisticated electronic device used primarily to care for ventricular tachycardia and ventricular fibrillation, two life-threatening abnormal heart rhythms. The ICD constantly monitors the center rhythm. When it detects a very fast, aberrant heart rhythm, it delivers energy to the heart muscle to crusade the heart to beat in a normal rhythm again.
Eye surgery – The Maze, modified Maze, and minimally invasive ablation surgeries are used to right atrial fibrillation that is not controlled with medications or not-surgical handling methods. Arrhythmia surgery also may exist recommended if you lot need surgery to right other forms of heart affliction (such equally valve illness or coronary artery disease).
Treatment likewise includes regular follow-upwardly with a physician. While women take specific concerns related to irregular heart rhythms, communication with your physician will ensure safe and effective treatment.
- Wolbrette D. Differences in the Proarrhythmic Potential of QT-prolonging Drugs. Current Women'due south Health Reports 2002, two:105-109.
- Karin H. Humphries, Charles R. Kerr, Stuart J. Connolly, George Klein, John A. Boone, Martin Greenish, Robert Sheldon, Mario Talajic, Paul Dorian, and David Newman. New-Onset Atrial Fibrillation : Sex Differences in Presentation, Treatment, and Consequence. Circulation 2001 103: 2365 - 2370.
- Bailey MS, Curtis AB. The Effects of Hormones on Arrhythmias in Women. Current Women's Health Reports 2002, two:83-88.
- Blacks, Women Less Likely to Get Implantable Defibrillators, world wide web.dukenews.knuckles.edu/2000/11/blackwomenheartn17.html .
Resources
Doctors vary in quality due to differences in training and experience; hospitals differ in the number of services available. The more than complex your medical problem, the greater these differences in quality become and the more than they matter.
Conspicuously, the doctor and hospital that you choose for circuitous, specialized medical care volition have a direct touch on on how well you do. To help y'all make this choice, please review our Miller Family unit Centre, Vascular & Thoracic Found Outcomes.
Cleveland Clinic Heart, Vascular & Thoracic Institute Cardiologists and Surgeons
Choosing a md to treat your aberrant middle rhythm depends on where yous are in your diagnosis and handling. The following Centre, Vascular & Thoracic Institute Sections and Departments treat patients with Arrhythmias:
- Section of Electrophysiology and Pacing: cardiology evaluation for medical management or electrophysiology procedures or devices - Call Cardiology Appointments at toll-free 800.223.2273, extension 4-6697 or request an engagement online.
- Department of Thoracic and Cardiovascular Surgery: surgery evaluation for surgical handling for atrial fibrillation, epicardial pb placement, and in some cases if necessary, pb and device implantation and removal. For more information, please contact u.s.a..
- MyConsult Online Second Opinion Service.
The Heart, Vascular & Thoracic Found has specialized centers to treat sure populations of patients:
- Atrial Fibrillation Eye
- Ventricular Arrhythmia Center
- Inherited Arrhythmia Clinic
Learn more about experts who specialize in the diagnosis and handling of arrhythmias
For younger patients with aberrant center rhythms:
- Visit The Middle for Pediatric and Congenital Heart Diseases web site
- Find a pediatric cardiologist
See Well-nigh Us to larn more about the Sydell and Arnold Miller Family Heart, Vascular & Thoracic Institute.
Contact
If yous demand more information, click hither to contact us, conversation online with a nurse or call the Miller Family Middle, Vascular & Thoracic Found Resource & Information Nurse at 216.445.9288 or price-gratis at 866.289.6911. Nosotros would be happy to help you.
Becoming a Patient
- Make an appointment
- Plan Your Visit
- Billing & Insurance
- Visitor Amenities
Treatment Options
- Arrhythmia Treatments
Handling Guides
- Atrial Fibrillation
- Ventricular Tachycardia
- All Miller Family unit Heart, Vascular & Thoracic Constitute Handling Guides
Diagnostic Tests
Diagnostic tests are used to diagnose your aberrant heartbeat and the most effective treatment method.
- Diagnostic testing
Beefcake
- How the heart beats
- Your heart and blood vessels
Webchats
Our webchats and video chats give patients and visitors another opportunity to ask questions and interact with our physicians.
- Abnormal Middle Rhythm webchats and video chats
- All Miller Family Heart, Vascular & Thoracic Institute webchats
Videos
- Center Rhythm Disorders and Treatments Videos
- All Miller Family Center, Vascular & Thoracic Found Videos
Interactive Tools
- Miller Family Heart, Vascular & Thoracic Institute Interactive Tools
Resource Links
- Recovery at abode
- Support Groups and Information
- Visit Wellness Essentials - Read articles on rhythm disorders and healthy living on Wellness Essentials
- Follow Heart, Vascular & Thoracic Constitute webchats and news stories on Twitter
- Subscribe to Centre, Vascular & Thoracic eNews
References
- Zipes, Douglas et al. Adult in Collaboration With the European Heart Rhythm Association and the Heart Rhythm Gild. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Study of the American College of Cardiology/American Centre Clan Chore Force and the European Gild of Cardiology Committee for Practise Guidelines *, *J Am Coll Cardiol* 2006 48: e247-346.
- Center Rhythm Social club. "Center Rhythm Disorders." Retrieved on March one, 2011, from HRS website: https://www.hrsonline.org/patient-resource .
- Heart Rhythm Society. "Skipped Heartbeats." Retrieved on March i, 2011, from HRS website: https://www.hrsonline.org/skipped-beats .
- The Merck Manuals Online Medical Library. "Ventricular Premature Beats (VPB)." Retrieved on March one, 2011, from Merck Manuals website: www.merckmanuals.com/home/centre-and-blood-vessel-disorders/abnormal-heart-rhythms/ventricular-premature-beats .
Why choose Cleveland Clinic for your intendance?
Our outcomes speak for themselves. Delight review our facts and figures and if you have any questions don't hesitate to ask.
Source: https://my.clevelandclinic.org/health/diseases/17644-women--abnormal-heart-beats
0 Response to "My Heart Beats Then There Is a Large Pause Then It Goes Back to Beating Normally Again"
Enviar um comentário